(TX_CURR_NAT) Percentage of people living with HIV receiving antiretroviral therapy
Export Indicator
ART coverage is the second 90 of the global target, and an important step in ending the AIDS epidemic. Antiretroviral therapy has been shown to reduce HIV-related morbidity and mortality among those living with HIV, and onward HIV transmission. Studies have also shown that early initiation, regardless of an individual’s CD4 cell count, can enhance treatment benefits and save lives, and WHO currently recommends treatment for all. The percentage of adults and children receiving antiretroviral therapy among all adults and children living with HIV provides a benchmark for monitoring global targets over time and comparing progress across countries. It is one of the 10 global indicators in WHO’s 2015 Consolidated strategic information guidelines for HIV in the health sector.
This indicator is harmonized with GAM indicator “People living with HIV on antiretroviral therapy.” However, the LTFU definition change is still being harmonized across all multilateral HIV organizations.
Given the shift in the definition of LTFU, it’s imperative that country teams use the host country indicator narrative to describe what definition is being used for TX_CURR reporting. Does the host country result assume a LTFU definition of <28 days or <90 days?
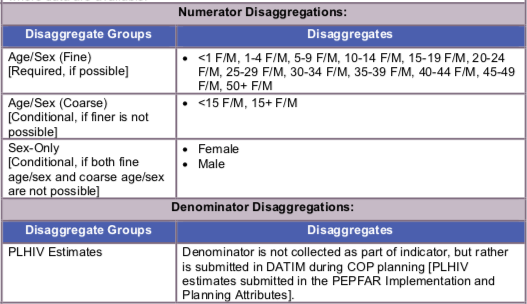
Number of PLHIV on ART at the end of the reporting period
Number of people living with HIV (PLHIV Estimate)
How to collect:
This indicator measures the progress towards providing antiretroviral therapy to all people living with HIV. The data source for this indicator is ART program monitoring tools, such as ART patient registers, pharmacy dispensing records, and summary reporting forms.
The number of adults and children receiving treatment can be obtained through data from facility- based antiretroviral therapy registers or drug supply management systems. Data should be collected continuously and aggregated on a monthly or quarterly basis to obtain subnational and national totals. The most recent full year of data should be used for annual reporting. Data should be collected from health facility recording and reporting forms, program data, health information system.
This indicator can be generated by counting the number of adults and children receiving antiretroviral therapy at the end of the reporting period. This value should equal the number of adults and children who have ever started antiretroviral therapy minus those not currently on treatment prior to the end of the reporting period. This will exclude those who died, stopped treatment or were lost to follow-up during the year.
Some people pick up several months of antiretroviral medicines (ARVs) at one visit, which could cover the last months of the reporting period. Efforts should be made to include these people in the numerator as receiving antiretrovirals even if they do not attend the clinic in the last month of the reporting period.
When disaggregating the numerator by age, people receiving antiretroviral therapy should be reported in the relevant age category based on their age at the end of the reporting year. HIV- positive pregnant women who are on antiretroviral therapy should be included in the numerator.
People receiving antiretroviral therapy in the private and public sectors should be included where data are available.
Reporting level: National and Sub-national: Data should be entered for all SNUs, regardless of PEPFAR- funded support for these geographical areas; so that the total of the sub-national number should equal the total number of national number.
Reporting frequency: Annually
Indicator changes (MER 2.0 v2.3 to v2.4): Narrative questions updated to address shift in lost-to-follow-up definition change
Data entered by: This data should be entered in DATIM by the USG country team.
Guiding narrative questions:
- Does the host country TX_CURR result assume a LTFU definition of <28 days or <90 days? Describe the data systems and methods of aggregation used at the national and subnational levels to report treatment data.
- Outline any work that the host country government has done to ensure that the reported figures are accurate (i.e., data quality assessments, results adjustment, etc.).
- Discuss progress towards aligning host-country age/sex disaggregations to standard five-year age and sex bands?
- For targets, please describe the host country target setting process.